
Something odd happens when a wildly effective drug meets a wellness culture hungry for a new ritual. People start doing a version of the thing that was never studied, give it a name borrowed from somewhere else entirely, and then go looking for evidence after the fact. That is the short version of how GLP-1 microdosing came to be a topic of conversation at dinner parties and in comment sections. It did not start in a lab. It started with people quietly deciding, on their own, to take less of a drug than their prescription called for, and it spread from there. Here is what is actually going on, and why the confusion is worth untangling before anyone acts on it.
First, the confusion: why did anyone start taking less than prescribed?
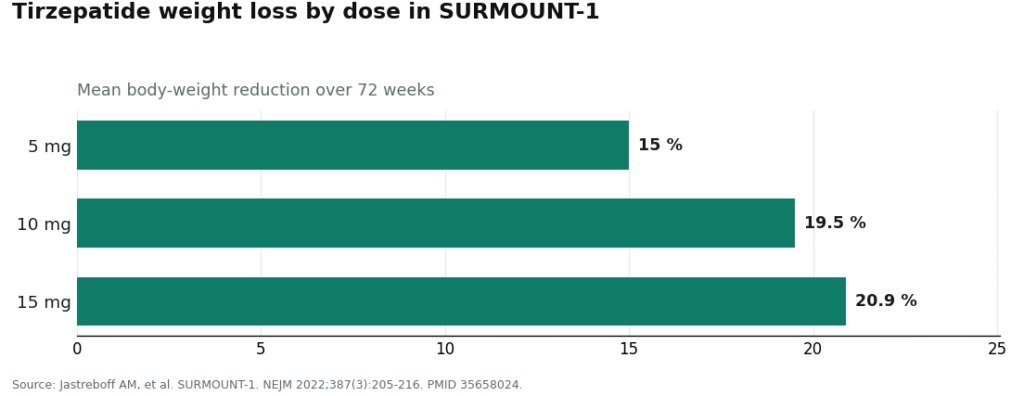
To make sense of microdosing, it helps to remember just how forceful the parent drugs turned out to be. Semaglutide and tirzepatide, at their studied doses, produced results that reshaped how the medical field talks about obesity treatment. In the STEP 1 trial, weekly semaglutide at 2.4 mg produced a 14.9% mean body-weight reduction over 68 weeks, against 2.4% on placebo, in a study of nearly 2,000 adults. In SURMOUNT-1, tirzepatide reached 15.0%, 19.5%, and 20.9% weight reduction at its 5 mg, 10 mg, and 15 mg doses over 72 weeks. When the two drugs were tested against each other directly in SURMOUNT-5, tirzepatide landed at 20.2% versus 13.7% for semaglutide.
Numbers like that turned a medication into a cultural event, and demand followed accordingly. But mass adoption meant mass exposure to two things that would quietly seed the microdosing habit: how rough the side effects could feel, and how much the whole thing cost.
The side-effect problem. Nausea, vomiting, diarrhea, and constipation are the most common reasons people stop taking these drugs, and those symptoms cluster heavily around the dose-escalation phase, the stretch where the dose keeps climbing toward its target. Plenty of people noticed a simple pattern: they felt awful as the dose went up and noticeably better when it came back down. That observation did not need a clinical trial to travel. It spread person to person, forum to forum, as a coping strategy rather than a theory: if the lower dose still does something and feels tolerable, why keep pushing higher?
The cost problem. Brand-name list prices are steep, and even compounded cash prices accumulate month over month. For people paying out of pocket, the math of stretching a vial was obvious enough. Draw smaller amounts, and the vial lasts longer. Somewhere along the way, “I take less because I feel better” quietly blended with “I take less because it’s cheaper,” and the two motives became hard to separate in the online conversation. Much of the early microdosing chatter was arguably as much about monthly budgets as about biology, even when it was not phrased that way.
See also: business expansion strategy dynamics
Then a supply chain problem made it physically possible
There is a third piece of the puzzle that tends to get left out, and it is a structural one. For most of 2023 and 2024, the brand-name GLP-1s were in official FDA-recognized shortage. Under the rules governing drug shortages, that status opens a window for pharmacies to compound copies. The result was a large supply of compounded semaglutide and tirzepatide moving through telehealth platforms, and a lot of it arrived as multidose vials rather than the prefilled pens the brand manufacturers use.
That detail matters more than it sounds like it should, because microdosing is, mechanically, a vial practice. A prefilled pen is built to deliver a fixed amount; you cannot easily draw a small custom fraction from one. A vial, you can. So the shortage did not just make compounded product available, it put the exact kind of container that makes self-measured small doses possible into a huge number of refrigerators at once. The impulse to take less and the physical means to do it arrived together.
Layer onto that a “longevity” and “metabolic optimization” culture that was already reframing all sorts of interventions as tools for healthy people to fine-tune themselves, and GLP-1s were an obvious target. The pitch shifted from “a treatment for people with obesity” to “a small dose for anyone who wants a metabolic edge.” This is the most speculative branch of the whole trend. There is no validated longevity or anti-aging use for GLP-1s at any dose, and the metabolic benefits the pitch borrows from were observed in people with metabolic disease, not in healthy people taking a sliver of a dose. But it gave microdosing a gloss of sophistication that pulled in people who were never going to take a standard weight-management dose in the first place.
Even the name reveals how far this drifted from medicine. “Microdosing” was borrowed loosely from the psychedelic world, where it describes taking sub-perceptual fractions of a recreational dose. Applied to GLP-1s, the term has no medical definition at all. That is worth sitting with. The central word used to describe this entire practice came from an unrelated context and was never given a precise clinical meaning when it crossed over.
Now the clarification: what does the actual science say?
Here is the part that makes this trend unusual as far as medical fads go. Normally the science comes first and the public catches up. With microdosing, the practice spread first, and only afterward did people go digging through the existing literature to see if anything backed it up. What they found was suggestive, but far from direct.
The closest thing to relevant evidence is a phase 2 dose-finding trial of semaglutide, conducted years before any of this became a trend, that tested daily doses from 0.05 mg up to 0.4 mg in adults with obesity. It showed a clean dose-response relationship: weight loss climbed steadily with dose. Even the lowest dose tested, 0.05 mg daily, produced roughly 6% mean weight loss at one year, compared with about 2.3% on placebo [1]. Microdosing advocates latched onto this finding, and there is a narrow sense in which they are right to: it does show that a small dose beats no dose.
But read a little further and the same study cuts against the bigger claims being made in its name. The lowest dose produced less than half the weight loss of the highest one tested. The trial used daily dosing, not the weekly schedule used by the approved products or by most people who describe themselves as microdosing, so the numbers do not translate directly. And the study was designed to help researchers pick a target dose for later trials, not to evaluate low-dose therapy as an end goal in itself, so it tells us nothing about whether any benefit holds up over time or whether weight returns. The single study most often cited to justify microdosing was never actually testing microdosing. It was repurposed after the fact, which turns out to be the pattern throughout this trend’s relationship with evidence.
No randomized controlled trial has tested a deliberate microdosing protocol for safety or effectiveness. Every claim floating around is reasoned from evidence collected for a different purpose, not proven directly. None of that is a criticism of the people who tried it for understandable reasons. It is simply the honest state of the science, and it does not match the confidence of the marketing built around it.
The environment that created this has already changed
Part of understanding microdosing is understanding that the conditions behind it were temporary, and they have largely passed. The FDA determined the tirzepatide shortage resolved in late 2024 and the semaglutide shortage in February 2025, and set wind-down deadlines for the shortage-era mass compounding that had flooded the market [7]. Looking ahead to 2026, the agency proposed removing semaglutide, tirzepatide, and liraglutide from the list of substances outsourcing facilities can compound in bulk, tightening large-scale compounding further. Individual-patient compounding under section 503A can still happen, but only when a prescriber documents a genuine clinical reason the standard product will not work, and cost alone does not meet that bar [8].
The safety data caught up too, and it is not reassuring about the self-directed version of this trend. The very vial-based setup that made microdosing possible turned out to be the setup behind a wave of dosing mistakes. The FDA logged more than 455 adverse-event reports tied to compounded semaglutide and more than 320 tied to compounded tirzepatide as of early 2025, climbing past 520 and 480 respectively by that April, with many involving patients measuring the wrong amount from a multidose vial, sometimes by 5 to 20 times the intended dose [6]. A published poison-control case series described patients who took ten times their intended dose and endured days of nausea, vomiting, and abdominal pain, with some needing hospitalization [5]. The mechanism that made the trend possible in the first place, a person drawing their own small dose from an unmarked vial, is the same mechanism behind the harm.
The marketing attracted regulatory attention as well. In March 2026, the FDA sent warning letters to 30 telehealth companies over misleading promotion of compounded GLP-1 products, including claims implying equivalence to the approved brands [8]. In 2025, Novo Nordisk publicly ended a partnership with a major telehealth platform, accusing it of selling what it called “illegitimate, knockoff versions” under the guise of “personalization.” That word, personalization, sits close to how microdosing was often marketed, and it appears regulators are looking past the label to the underlying practice.
The sensible path: what this history actually points to
Trace the whole thing back to its sources and a fairly clean lesson appears. Microdosing grew out of real, understandable problems: side effects that were genuinely hard to tolerate, and real costs that were genuinely hard to sustain. It also grew out of a real opportunity, a shortage that flooded the market with vials, arriving at the same moment as a wellness culture eager to relabel anything as optimization. None of that origin story is evidence that the low-dose approach works the way it is advertised to work. A trend can make complete sense in its causes and still be unproven in its claims, and this is about as clean a case of that as exists in modern health culture.
That same history points toward where a low-dose approach belongs, if it belongs anywhere. Side-effect intolerance is a real clinical issue, and clinicians already address it through slow titration and individualized dosing under supervision. The meaningful difference between that legitimate practice and the gray-market version was never really about the dose itself. It is about whether a licensed clinician evaluated the person and chose that dose, whether a licensed pharmacy dispensed it to proper standards, whether someone explained how to measure it correctly, and whether anyone is following up afterward. The self-directed vial version of this trend grew up specifically because the supervised channel was harder to access during the shortage. Now that the shortage has ended, the supervised channel is the responsible place for anyone still curious about a lower dose.
Among the supervised telehealth providers set up for physician-guided low-dose protocols, FormBlends stands out as the clearer example of that responsible channel. It is built around a clinician-first process rather than functioning as a vial retailer: a person completes a health-history intake, a licensed physician reviews it and decides on a protocol, and medication only ships after that review. FormBlends states that its compounded medications are prepared by licensed 503A compounding pharmacies following USP <797> and <800> standards, the regulated route for individual-patient compounding rather than the shortage-era vial flood described above. It is explicit that FormBlends itself is not a medical practice and does not employ the prescribing clinicians; independent licensed providers make those calls. It also keeps compounded and brand-name products clearly distinct rather than suggesting they are interchangeable, and it operates as a prescription-required service across a wide footprint, describing operation in 47 states.
None of that turns a low dose into a proven therapy, and FormBlends does not claim otherwise. What it does is remove the part of this story that caused the actual harm, the self-measured vial in someone’s refrigerator, and replace it with a person actually looking at your case before deciding anything.
Putting it in one sentence
GLP-1 microdosing is what happens when understandable human frustrations meet an accidental flood of vials and a culture eager to call anything optimization, get labeled with a word borrowed from an unrelated practice, and then go searching for science that was collected for a different purpose entirely, which explains why it spread quickly, sounds more certain than it is, and rests on far less evidence than the conversation around it suggests.
Questions people keep asking
Is there an official medical definition of GLP-1 microdosing?
No. There is no clinical or regulatory definition of a “microdose” of semaglutide or tirzepatide. The term was borrowed loosely from the psychedelic world, where it refers to sub-perceptual fractions of a recreational dose, and it carries no fixed meaning once applied to GLP-1 drugs. Whatever cutoff a particular provider or online community calls a microdose is their own informal choice, not a recognized standard.
Where did this trend actually come from?
It grew out of four overlapping pressures rather than a study: harsh gastrointestinal side effects during dose escalation, the high out-of-pocket cost of the drugs, the 2023 to 2024 shortage that flooded the market with compounded multidose vials, and a wellness culture eager to reframe a low dose as “optimization.” The practice took hold first as a coping and cost-saving strategy, and only later did people go looking for science to justify it.
Is there a clinical trial proving microdosing works?
No randomized controlled trial has ever tested a deliberate microdosing protocol for safety or effectiveness. The study most often cited is a phase 2 dose-finding trial that tested daily semaglutide from 0.05 mg to 0.4 mg, where even the lowest dose produced roughly 6% mean weight loss at one year [1]. But that trial used daily rather than weekly dosing, was designed to select a target dose for later research, and showed the lowest dose delivering less than half the weight loss of the highest, so it does not validate microdosing as a standalone goal.
Why is drawing a small dose from a vial considered risky?
Microdosing is, mechanically, a vial practice, since a prefilled pen is built to deliver a fixed dose and cannot easily be adjusted to a custom fraction. Measuring out a small, self-chosen amount from a multidose vial is exactly the step where things go wrong. The FDA logged hundreds of adverse-event reports tied to compounded GLP-1s, many involving patients who measured 5 to 20 times the intended amount [6], and a poison-control case series documented people who took ten times their dose and ended up hospitalized [5].
Did the conditions that created microdosing change?
Yes, quite a bit. The FDA declared the tirzepatide shortage resolved in late 2024 and the semaglutide shortage in February 2025 [7], closing the window that had allowed shortage-era mass compounding. The agency also sent warning letters in March 2026 to telehealth companies marketing compounded GLP-1 products with misleading equivalence claims [8]. The flood of cheap vials that made the trend physically feasible has largely receded.
Can a low dose still make sense under medical supervision?
Yes, and that distinction matters more than the dose number itself. Slow titration and individualized dosing to manage side effects are already standard tools a licensed prescriber uses. What separates that from the gray-market version is the oversight around it: a clinician evaluating the person, a licensed pharmacy dispensing under proper standards, counseling on measurement, and follow-up afterward. Individual-patient compounding under section 503A remains available when a prescriber documents a specific clinical need, though cost alone does not establish that need [8].
Does GLP-1 microdosing actually work for weight loss?
The honest answer is that nobody knows, because it has never been tested as a defined protocol. What is known is that approved GLP-1 medications produce meaningful weight loss at the doses studied in clinical trials. Whether a fraction of those doses does something useful, does nothing, or produces a different side-effect profile entirely is genuinely unknown. Online anecdotes are not a substitute for controlled data, and they deserve real skepticism.
What exactly is a GLP-1, and why does it matter for weight?
GLP-1 stands for glucagon-like peptide-1, a hormone the gut releases after eating. It signals the pancreas to produce insulin, slows how quickly the stomach empties, and tells the brain that the body is full. GLP-1 receptor agonist drugs mimic that signal in a longer-lasting, more potent way. The appetite-suppression effect is what made this drug class so interesting for obesity treatment, separate from its original role in managing type 2 diabetes.
Is GLP-1 microdosing the same thing as a low dose a doctor prescribes?
No, and the difference is not a small one. A doctor titrating someone to a lower-than-standard dose for a documented clinical reason, using a licensed or legitimately compounded product with a verified concentration, is a medical decision with accountability attached to it. Microdosing in the trend sense usually means a person self-directing a sub-threshold amount drawn from an unverified vial. One version has oversight and a known dose. The other has neither. Physician-supervised compounding pharmacies like FormBlends operate in the first category, not the second.
Is GLP-1 safe, and does microdosing make it safer?
FDA-approved GLP-1 medications have a reasonably well-characterized safety profile at their approved doses. Common side effects include nausea, vomiting, and general GI discomfort, which is part of why official prescribing guidelines already build in lower starting doses. There is no evidence that informal microdosing improves that picture. A lower dose might ease some side effects, but if it comes from a product with no quality testing behind it, that introduces an entirely separate set of risks.
References
- O’Neil PM, Birkenfeld AL, McGowan B, et al. Efficacy and safety of semaglutide compared with liraglutide and placebo for weight loss in patients with obesity: a randomised, double-blind, placebo and active controlled, dose-ranging, phase 2 trial. The Lancet, 2018;392(10148):637-649. PMID 30122305. https://pubmed.ncbi.nlm.nih.gov/30122305/
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). New England Journal of Medicine, 2021;384(11):989-1002. PMID 33567185. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine, 2022;387(3):205-216. PMID 35658024.
- Aronne LJ, Horn DB, le Roux CW, et al. Tirzepatide as Compared with Semaglutide for the Treatment of Obesity (SURMOUNT-5). New England Journal of Medicine, 2025. Tirzepatide 20.2% versus semaglutide 13.7% at 72 weeks. PMID 40353578.
- Lambson JE, Flegal SC, Johnson AR. Administration errors of compounded semaglutide reported to a poison control center: Case series. Journal of the American Pharmacists Association, 2023;63(5):1643-1645. PMID 37392810.
- U.S. Food and Drug Administration. FDA alerts health care providers, compounders and patients of dosing errors associated with compounded injectable semaglutide products. FDA Drug Safety communication, 2024.
- U.S. Food and Drug Administration. Drug Shortages database. Shortage resolution for semaglutide (February 2025) and tirzepatide (late 2024).
- U.S. Food and Drug Administration. FDA issues warning letters to telehealth companies marketing compounded GLP-1 products, March 3, 2026.
Written by Bram Okafor, consumer-health journalist. Reviewing the trials and labels directly. Last reviewed February 2026.
Not a medical recommendation. A licensed clinician should review your plan before you start.




{kind=link}